
Some two hundred miles northeast of the Nigerian capital, Abuja, two-year-old Mohammad Sheriff is on the road to recovery from cholera. The boy sits with his father in a cholera treatment center (CTC) run by Doctors Without Borders/Médecins Sans Frontières (MSF)in Bauchi, the capital of one of the states hit hardest by Nigeria’s worst cholera outbreak in a decade. This year, the country has seen more than 90,000 people infected so far. MSF emergency teams are working alongside the Nigerian Ministry of Health to bring the spiralling outbreak under control, opening six cholera treatment centers across the region and treating more than 20,000 patients so far.
“He vomited twice and later started having diarrhea,” said Sheriff’s father, who immediately recognized the symptoms as cholera. “I told his mother that I'd take him to the hospital, as we are constantly being informed through the radio that one should immediately go to hospital when vomiting and diarrhea starts.”
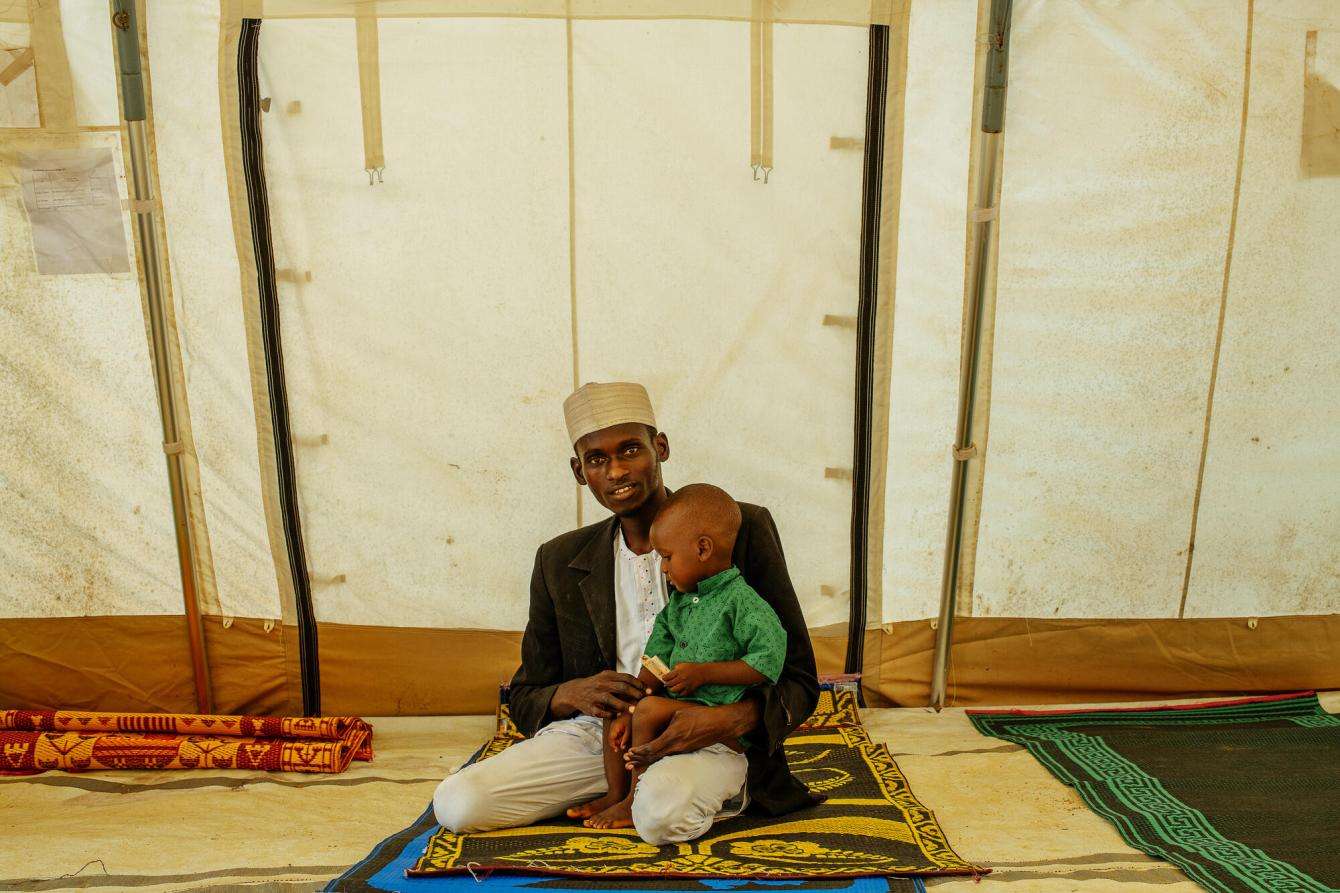
Sheriff’s case was serious, but after two days receiving medical care in the CTC, he is now in the recovery ward—the last step before being discharged and returning home. “If we had not come when we did, the situation might be very bad,” his father said.
Cholera is simple to treat in most cases, and people with mild to moderate forms of the disease usually recover through treatment with fluids and oral rehydration solution. Severely dehydrated patients may need to be admitted to a CTC and be given fluids intravenously.
While nearly all of Nigeria’s thirty-five states have reported cholera cases in 2021, the vast majority have been concentrated in the six northern states of Bauchi, Kano, Jigawa, Zamfara, Sokoto, and Katsina. Many people in this region are particularly vulnerable—hundreds of thousands have been displaced from their homes by conflict and violence, and many live in conditions with poor sanitation and without safe drinking water.
In many areas, security poses an additional challenge. In Zamfara state, many patients arrive for care in a serious or critical condition because they delayed seeking treatment because conflict has made travel extremely dangerous. Despite this, MSF teams were still admitting more than 100 patients a day in August, underscoring the severity of the outbreak and the determination of patients to get treatment, however risky.
“Vulnerable people in Nigeria were already in a dire situation,” said Dr. Simba Tirima, MSF country representative in Nigeria. “Cholera has added to a complex web of medical and humanitarian vulnerabilities, coming on top of heightened insecurity, a chronic state of acute humanitarian and medical needs, and the direct and secondary impacts of COVID-19.”
At the peak of the outbreak in July, the Nigerian Center for Disease Control reported more than 7,500 new cases per week and many medical facilities were at risk of being overwhelmed.
“We had to admit 80 or 90 patients during a single work shift,” says Anas Al-Hassan, a nurse at MSF’s CTC in Kano, where the outbreak spread quickly throughout the community. “There was no time for rest because of the number of patients. The work at that time was overwhelming.”

“The patients would come devastated, their caregivers worried they might not make it,” said Philip Esenwa, MSF medical activity manager for the Nigeria Emergency Response Unit. “Some were so weak that they couldn’t speak.”
Some people were brought in after they had already died, said MSF nurse supervisor Mustapha Mahmud, who also works at Kano CTC.
Many medical facilities in these areas were not equipped to deal with the surge in patients. Some private facilities charge for their services, which puts treatment out of reach for those who cannot afford to pay.
The challenges were immense in cities such as Kano and Bauchi, where many people live in overcrowded conditions, with poor or nonexistent sewage systems and no access to clean drinking water. Water sources can easily become contaminated with sewage, especially in the rainy season, causing waterborne diseases such as cholera to spread quickly.
“The areas with high numbers of cholera cases are congested, with no adequate ventilation or proper drainage,” says Mahmud. “The sources of water are usually from shallow wells and boreholes. With rainfall, they become contaminated, and that is the water people here drink.”
To grapple with these complex challenges, MSF adopted a community-based approach, taking health care, hygiene measures, and public health information directly to the affected communities. MSF health promotion teams worked with Ministry of Health staff to conduct door-to-door contact tracing to find people with symptoms and help them get medical care quickly, while outreach teams chlorinated wells and disinfected patients’ homes.

Working with community leaders, MSF teams also identified neighborhoods with high concentrations of cases to set up oral rehydration points, where patients with milder symptoms could receive treatment.
In some states, a one-dose oral vaccine is available to help reduce the spread of the disease. However, global supply is limited and the vaccine is not available everywhere.
In the areas where MSF is responding, these and other efforts have made a difference. In Bauchi state, where MSF set up 19 oral rehydration points and a cholera treatment unit and carried out health promotion and hygiene activities, the mortality rate has been reduced by a factor of ten, from 5 percent to less than 0.5 percent, and the number of new patients being admitted for treatment continues to decline.
The trend of declining cases holds true for the country overall, with new cases in recent weeks falling to below 1,000 per week from a peak of 7,500. In many areas, this has brought a sense of relief for communities and medical teams alike.
“Thankfully, there has finally been a significant decline in the number of new cases in most areas,” says Dr. Tirima. Elsewhere in the country, however, the outbreak rages on. “Other areas continue to be affected and the response is not over yet,” he warns.
One of those areas is Borno state, where hundreds of thousands of people have been displaced from their homes by clashes between government forces and armed groups. Years of conflict and displacement have left people struggling to access clean water and sanitation. In the state capital, Maiduguri, the MSF team continues to treat nearly 200 patients per week for cholera and acute watery diarrhea.
In March 2021, MSF launched a cholera response in Gusua, in northwestern Nigeria’s Zamfara state, setting up a 30-bed cholera treatment unit (CTU), which closed in late-July. In May 2021, MSF set up three cholera treatment centers (CTCs) in Kano and Bauchi states: a 130-bed CTC in Kano and a 40-bed CTC in Tambaruwa, both in Kano state; and an 80-bed CTC in Bauchi state; all are now closed. As the epidemic continued to spread in August, MSF opened four more CTCs in Zamfara and Borno states: a 72-bed CTC in Anka, a 30-bed CTC in Shinkafi and a 68-bed CTC in Zurmi, all in Zamfara state; and a 40-bed CTC in Maiduguri, Borno state; these CTCs remain open. MSF also managed eight CTUs and 25 oral rehydration points across northern Nigeria; most of these are now closed.
MSF has been working in Nigeria since 1996.
